
TUBERCULOSIS (TB)
TB is a disease, caused by Mycobacterium tuberculosis bacteria (MTB). TB usually affects the lungs, as chronic pneumonia, but may affect almost any body organs.
Terminology:
ACID FAST BACTERIA (AFB):
Another description of the MTB is Acid Fast Bacteria (AFB).
Acid Fastness is due to the high amount of the glycolipid, mycolic acid, in their capsular walls, which when stained red with carbofuchsin, resist subsequent acid decoloration.
At the tissue level, the hallmark of TB infection is tubercles (granuloma) which are round nodules with macrophages in the center, surrounded by lymphocytes.
SPREAD OF MTB
The MTB is transmitted through air, either
a.) directly, when a person with active TB, (in the lungs or throat) expels the germs into the air, (by coughing, spitting or sneezing), within 1-2 meters of another person, who then inhales the bacilli into their lungs.
b.) indirectly by inhaling airborne dust and particles containing the TB bacilli.
TB bacteria is killed by Ultraviolet light and sunlight, so transmission usually occurs indoors
Transmission usually occurs, where people share a single, indoor space, for prolonged periods, example, prisons, shelters, between family members, co-workers and close contacts.
The bacilli may also be transmitted through breaks in the skin.
Infectious Dose: Inhalation of 10 bacilli is enough to cause infection.
SURVIVAL OF MTB OUTSIDE OF THE BODY:
MTB is killed by Ultraviolet light and sunlight, so transmission usually occurs indoors. UV light denatures the bacteria's DNA, can be used for surface disinfection
Mycobacteria are easily killed by heat greater than 65*C for at least 30 minutes
The bacteria can survive in droplets and particles, protected from UV-light, for long periods. Droplets are light, and may remain suspended in rooms for ,4-6 hours and then die;
MTB survives in sputum on carpets (19 days), in the soil (4 weeks-4months) and in dark environments (74 days)
MTB is not spread by
. Shaking hands, or Kissing
. Sharing food or drinks, toothbrushes and clothes
. Using a toilet
LATENT TB INFECTION:
After inhalation, the bacilli, settle, usually, in the lungs where the body's defenses, build a wall of cells around the bacilli, to contain it. Without medication the bacteria are not eliminated from the body, and the individual can develop an active and severe disease, at a later date.
Persons with latent TB, are not sick and they do not have symptoms. They however, produce immune cells and biologic agents to block the spread of the germs.
ACTIVE TB INFECTION:
When the body's immune system, is unable to contain the bacilli, the MTB are able to grow and spread to other parts of the lungs and the rest of the body.
About 5-10% of persons with latent TB, who do not receive preventive treatment for it, will develop active TB infection and become sick.
INCUBATION PERIOD:
Incubation period is 4-6 weeks, in most cases.
5% of infections progress to active TB within the first 2 years. Other infected persons still have 5-10 % chance of converting to active TB during their lifetime.
Some people are known for their higher risk of developing active TB
PERSONS AT HIGHER RISK FOR ACTIVE TB
. Persons infected with HIV (highest risk factor), are 20-30 times more likely to develop active TB.
. Infants and children less than 4 years.
. People infected within the last 2 years
. Others with impaired immunity, like
. Diabetics,
. Chronic kidney diseases,
. Tobacco smokers do have much higher risk of developing active disease.
SYMPTOMS OF ACTIVE TB.
General Symptoms:
Feeling weak or sick
Poor weight gain or weight loss (failure to thrive in children)
Lack of appetite
Fever
Night sweats.
SYMPTOMS RELATED TO ACTIVE LUNG TB:
. Chronic cough (longer than 3 weeks)
. Chest pain on coughing or while taking deep breaths.
. Coughing up blood or phlegm
DISSEMINATED TB (MILIARY TB)
Disseminated TB is characterized by
. Persistent High Fever
. Malaise
. Night sweats. cough
. Enlarged spleen and enlarged lymph nodes
About half of persons with miliary TB develop brain involvement manifesting as focal weakness and altered mentation
TB AFFECTING OTHER PARTS OF THE BODY
Bladder: pus in urine on microscopy
Kidneys: blood in urine
Spine: back pain and spinal deformity
DIAGNOSIS OF TB INFECTION.
Once the germ enters the body, the body's immune systems produce cells and biological agents to contain the germs, (starting 2-12 weeks after inhalation). The body's reaction to TB bacilli, enables scientists to perform TB-screening tests:
1.) Tuberculin skin test(TST)
0.1ml of tuberculin (purified protein derivative), is injected into a forearm skin, and reactions are read 48-72 hours later. If the body's immune cells react to the antigen, as indicated by skin induration (not redness) of 10mm diameter, it is labeled as positive TST. For persons with HIV infection, those with recent contact with TB patients, or those on certain medications that decrease immune responses, a diameter greater than 5mm is positive TST.
An induration with a diameter less than 5mm is read as Negative
A TST may be falsely read negative, if TB infection is recent (within 8-10 weeks of exposure) or after viral infections and in kids less than 6months old.
2.) Interferon Gamma Release Assays (IGRA)
This is a blood test that detect biologic agents released by T-lymphocytes in response to TB infection.
IGRA testing may be done in place of TST, but IGRA is preferred for the following conditions:
a.) persons who have had BCG vaccinations, (a prior BCG vaccination has no effect on IGRA.)
b.) persons who may not return within 48-72hour window for the test reading.
NB: TST is preferred over IGRAs for testing children less than 5 years of age.
Quantiferon TB-gold and T-SPOT-TB are the two IGRA tests available
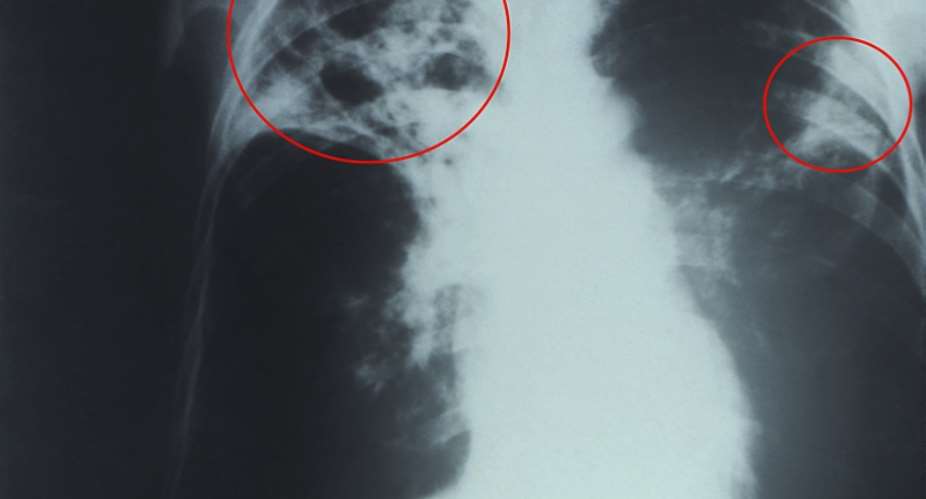
3. Chest X ray (CXR)
A CXR is done for positive screening test results. CXR shall determine latent or active lung infection.
4.) Sputum Nucleic acid Amplification MTB test (sputum NAAT for TB)on persons with a positive AFB sputum smear may help in starting TB treatment early, but it does not tell the sensitivity of MTB to TB-medications.
5.) Sputum culture for AFBs, (90% sensitivity) requires several weeks of growth, before results become available.
TREATMENT
TB infection is treatable and curable.
FIRSTLINE-MEDICATIONS:
Isoniazid (INH)
Pyrazinamide (PZA) (Avoid PZA in pregnancy)
Rifampin (RIF)
Rifabutin
Rifapentine
Ethambutol (EMB)
SECOND-LINE MEDICATIONS
Streptomycin
Cycloserine
Capreomycin
Ethionamide
Kanamycin
Amikacin
Levofloxacin
Moxifloxacin
Para-aminosalicylic acid
Bedaquiline
TREATMENT OF ACTIVE TB
For initial treatment, INH, RIF, PZA and EMB are taken daily for 8 weeks (56 doses), followed by 18 weeks (126 doses) treatment with INH+RIF
TREATMENT OF LATENT TB (PREVENTION OF ACTIVE TB)
INH daily for 9 months, or
INH + RIF once a week for 12 weeks
DRUG-RESISTANT-TB
TB Drug resistance is common in people who
. Do not take their TB medications exactly as directed. They take the medications, irregularly, on and off.
. Become infected with TB strains that have become resistant TB medications.
When MTB is resistant to both RIF + RIF, (the 2 most potent TB medications), the term multidrug-resistant tuberculosis (MDR TB) is used
When MTB is resistant to RIF+ INH + (Levofloxacin or Moxifloxacin) + any of the TB injections (capreomycin, Amikacin or Kanamycin), the term: Extensively drug resistance TB (XDR TB) is used.
For resistant MTB, bedaquiline (sirturo),for adults or delamanid (Deltyba) for those older than 6 years of age, are added to at least, 3 other anti-MTB medications.
Bedaquiline and Delamanid are administered daily for 24 weeks or more. Administration requires direct monitoring and close consultation with TB specialists due to their many adverse effects. Monitoring continues for 2 years
CRITERIA FOR CONSIDERATION AS "NO LONGER INFECTIOUS".
Persons with active TB and positive AFB smears must
. cover their mouths when coughing
. spend more time outdoors.
. Sleep alone in well ventilated, sunlit rooms.
. Avoid crowded places and public transportation.
Persons with active TB are considered non-infectious if the following 3 conditions are met.
. Adequate treatment was started more than 2 weeks ago.
. Improvement in symptoms
. 3 consecutive, (early morning) AFBs sputum smears are all negative.
PREVENTION OF TB INFECTION
BACILLE-CALMETT-GUERIN (BCG):
A live-attenuated, Bovine-TB derived; MTB Vaccine may prevent disseminated TB and TB meningitis in children, but not in Adults. BCG vaccine may be considered in all TST-negative children who are at risk for getting MTB (both sensitive and drug-resistant MTB) infection.
For those with latent TB: INH daily for 9 months, or INH + RIF once a week for 12 weeks
PREVENTION OF DRUG RESISTANT TB
. Take all TB medications as directed by Doctors and other health authorities
. Don’t miss or stop taking TB medications, until you discuss it with the doctor
 Western North been sidelined for far too long; address our needs before 2024 ele...
Western North been sidelined for far too long; address our needs before 2024 ele...
 Effutu: 'Stop eating at night and take care of your health' — Afenyo Markin advi...
Effutu: 'Stop eating at night and take care of your health' — Afenyo Markin advi...
 Akufo-Addo's desperate attempt to disrupt Yagbonwura's 1st year anniversary cele...
Akufo-Addo's desperate attempt to disrupt Yagbonwura's 1st year anniversary cele...
 Armed robbers attack, rob Sethi Brothers Ghana Limited in Tema
Armed robbers attack, rob Sethi Brothers Ghana Limited in Tema
 SML deal: We commend Manasseh for holding gov't to account, Akufo-Addo for not s...
SML deal: We commend Manasseh for holding gov't to account, Akufo-Addo for not s...
 Our recall invocation is in good faith to consider three key issues – Majority
Our recall invocation is in good faith to consider three key issues – Majority
 You’re inviting bad luck upon yourself if you use Indian hair — Spiritualist war...
You’re inviting bad luck upon yourself if you use Indian hair — Spiritualist war...
 Ejisu by-election: Police questions Kwadaso MP, two others over bribery allegati...
Ejisu by-election: Police questions Kwadaso MP, two others over bribery allegati...
 Nana Kwame Bediako is Nkrumah’s reincarnate; he’ll be president if he appoints N...
Nana Kwame Bediako is Nkrumah’s reincarnate; he’ll be president if he appoints N...
 Dumsor: Mahama gave us ‘dum, dum, dum’ but we are now in the era of ‘dum sie sie...
Dumsor: Mahama gave us ‘dum, dum, dum’ but we are now in the era of ‘dum sie sie...
