

Recently, I advised some clients who opted for alternative medicine to consider hormone treatment. Partly because; I realized, their PSAs were rising despite being on alternative medicine. I realized from their looks, the disappointment. But I told them, the advice is in their own interest. They were happier after I told them the program I have in place to help deal with the side effect of the hormone treatment to improve on their quality of life. Their confidence level finally went up! Most of my clients’ problem has to do with dealing with the side effect of conventional treatment; it is therefore prudent conventional cancer treatment have a program in place to improve quality of life. My aim is to provide objective information to my clients based on their cancer outlook to avoid preventable death. Not all men also benefits from alternative treatment for their prostate cancer, integrative approach have become very necessary.
So for men on hormone therapy; there is hope to help you deal with the side effect of the treatment to improve your quality of life and your general survival rate. I am not against conventional treatment; but I believe in friendly medicine: medicine based on science. Let’s look at this new hormonal drug approve for prostate cancer and what you have to do for being on hormone treatment for your prostate cancer.
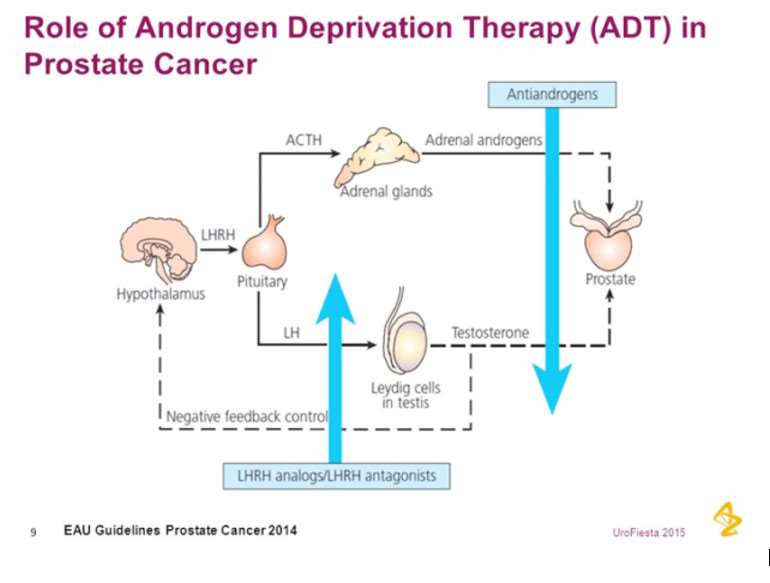
Hormone Deprivation Therapy
Hormone Deprivation therapy, also known as Androgen Deprivation Therapy (ADT) is a common long-term treatment for men with more serious prostate cancer or short-term therapy before undergoing radiation therapy. Either way, when a man’s testosterone levels go down to nearly zero, life is experienced differently.
According to Dr. Geo Espinoza; one of the world finest Naturopathic Urologist in the US “My partner, David at XY Wellness recalls when he was on short-term ADT before radiation nearly fifteen years ago;
“ ADT materially alters how you interpret and engage with the world around you. It taught me that there is far more than a mind-body connection by suggesting that they are one in the same.”
He continues;
“While undergoing ADT, it is not so much that the man is disinterested in sex but that it simply does not cross his mind.”
Apalutamide with the trade name Erleada…The New Product Approved!
Recently, Apalutamide, goes by its trade name Erleada was approved for treating men with rising PSA (recurrence) after treatment for prostate cancer without metastasis. Currently, this is the first standard treatment for a scenario for a rapidly rising PSA without metastasis.
The Research on Apalutamide
The study involved a total of 1207 patients who underwent randomization: 806 were assigned to the Apalutamide group(240 mg per day) and 401 to the placebo group in the phase 3 SPARTAN (Selective Prostate Androgen Receptor Targeting with ARN-509) trial
NOTE: It is common for there to be funky names to large trials like other ADT studies; LATITUDE, CHAARTED, etc. It helps physicians (especially when lecturing) and lay people alike mention the studies with ease. Of course, SPARTAN has a warrior kind of implication… as in, are you ready to fight? Clever.
Follow up research
In the follow up study for close to two years, the Study participants had confirmed prostate cancer that was castration-resistant and was at high risk for the development of metastasis, which was defined as a PSA doubling time of 10 months or less during continuous androgen-deprivation therapy. Patients with evident bone metastasis were excluded from the study. The results revealed that: Time to metastasis, progression-free survival, and time to symptomatic progression were significantly longer (70% better) with Apalutamide than with placebo. Apalutamide was associated with higher rates of rash, fatigue, joint pain, weight loss, falls, and fracture than placebo.
Dr. Geo Espinoza takes on Apalutamide:
Apalutamide is an anti-androgen agent, meaning it lowers testosterone and Dihidrotestosterone (DHT) to almost zero, similar to other forms of Androgen Deprivation Therapy (ADT) except blocks the genetic formation of androgen receptors.
The study was paid for by Janssen Pharmaceutical, the developer of the drug. “I say this because when studies funded by the company that makes the drug questioned, the results are often favorable to the company sponsoring the product. Thus there seems to be some bias playing a role in such scenario”.
That said, the design of the study was good, and it was published in one of the most respectable journals, New England Journal of Medicine (NEJM), so I will proceed with a small air of caution.
Seventy percent improvement from cancer worsening in two years compared to placebo is darn good. Of course, no drug that works too well comes without downside (excuse the pun).
Men on Apalutamide showed higher rates of rash, fatigue, joint pain, weight loss, falls, and fracture than placebo.
Side Effects
Long-term treatment of ADT is associated with side effects, such as fatigue, reduced bone mineral density, increased fracture risk, decrease in skeletal muscle mass (muscle wasting), associated with the development of metabolic syndrome/insulin resistance, increase in adverse cardiovascular events effects and increases the risk of anemia, hot flashes, gastrointestinal tract disturbances, loss of libido, impotence, osteoporosis, gynecomastia, deep vein thrombosis, congestive heart failure, myocardial infarction, pulmonary edema, cognitive decline and psychological changes.
“As I continue to monitor the well-being of many prostate cancer patients on ADT, I can say with very little doubt that men can live long and strong while undergoing hormone therapy”.
With one caveat…If you must follow a lifestyle and exercise regimen that supports your body. Many of my patients on ADT are “crushing it” by doing so. Not only is prostate cancer successfully managed when combining ADT with lifestyle, but the quality of life is also exceptional. I am not exaggerating. Geo Espinoza provided a scenario between him and patient on ADT.
Should I be on ADT? What would you do if you were me? I’m often asked by patients, “What would you do if you were in my shoes? Would you go on ADT?” Such question reminds me of a line in one of the few books I read from cover to cover in high school (I wasn’t a big reader then), To Kill a Mockingbird by Harper Lee…“You never really understand a person until you consider things from his point of view until you climb inside of his skin and walk around in it.” In other words, I am not you. And I have not been diagnosed with PSA recurrence after initial treatment for prostate cancer with curative intent
That said, I do read many scientific papers on prostate cancer, have extensive clinical experience with patients battling this disease, and have opinions about prostate cancer treatments and quality of life.
Here’s his answer to the client…
“I am a sucker for a good quality of life. I’d choose the quality of life over longevity in most cases. Much would depend on the severity and length of time of adverse effects from ADT. Thus, every case is different. If God forbid, I am diagnosed with aggressive, stage 4 lung cancer; it is likely that I will choose no medical treatments as experience and data show not a significant survival rate and poor quality of life with the available treatments for such disease and numerous others alike. But I digress. We are talking about prostate cancer. Men on ADT in my practice are doing exceptionally well, likely because they are following my nutritional and exercise advice. Based on that experience, getting on ADT treatment for the right patient and the available data supporting its use in improving survival is a good option”.
Lifestyle practices to men with prostate cancer while on Hormone Deprivation Therapy or ADT
The premise of the lifestyle program for men on ADT is to:
- Review and implement the science related to food, exercise, and nutrition related to prostate cancer.
- Individualize the CaPLESS Method to the person’s specific type of prostate cancer and overall health.
- Make it sustainable, so the lifestyle is sustainable for life and not temporary.
Specific lifestyle recommendations for Men on hormone deprivation therapy
It is very important for men to practice some specific lifestyle programs whilst on ADT. Today we will talk about exercise, likely the most important components.
Exercise Prescription for men on Hormone Deprivation Therapy or Androgen Deprivation Therapy (ADT) to treat Prostate Cancer

The goal for men on ADT and applying lifestyle practices are:
- Minimize adverse and unwanted side effects from the treatment
- Create a hostile biological environment for cancer in the body
- Optimize quality of life despite the ADT
Wow! You may be wondering; that’s a lot. Can we accomplish all that? Yes, it is. And yes you can. The right lifestyle and exercise program like the CaPLESS method introduced by Dr. Geo Espinoza can minimize about 80% of those side effects. I am not kidding and have seen it all on prostate cancer! Prostate cancer related death is high in Ghana with lots of men suffering from side effects of conventional treatment; hence, my duty to save more lives by addressing the side effects with right programs. Low libido, impotence (or let’s call it sexual dysfunction. Impotence sounds a bit harsh) and hot flashes are non-life threatening and more difficult to treat. Most other side effects that are more life-threatening are greatly reduced.
Research on Exercise while on Hormone Deprivation Therapy or ADT.
In one study of 2,700 male health care professionals (average age 70 years) with non-metastatic prostate cancer and found that those participating in vigorous physical activity for a duration ≥3 hours/week demonstrated a 49% lower risk of all-cause mortality and a 61% lower risk of death specifically from prostate cancer, compared with men who did 1 1 hour/week of vigorous activity. (Kenfield et al. 2011)
A systematic review of ten studies (five randomized and five uncontrolled clinical trials) examined the effects of exercise on patients receiving ADT. This paper demonstrated that physical performance was improved by exercise. Randomized controlled trials found exercise to be consistently beneficial for muscular performance: reported as increases in muscular strength and increases in upper and lower limb strength, compared with the control population. (Gardner et al. 2014)
Body composition (the amount of fat vs. muscle in the body) is a component of many studies investigating exercise effects on prostate cancer patients on ADT and resistance training has been shown to either increase lean body mass or not decline. Loss of muscle mass is a common scenario amongst ADT patients. (Galvão et al. 2010). An observational study reported in 2006 looking at over 70,000 men observed 11% increase in myocardial infarction risk and a 16% increased risk of coronary heart disease and death from cardiac arrest in the study of prostate cancer patients receiving ADT, versus those not on hormone therapy. (Keating et al. 2006)
We would want to avoid those cardiovascular problems, right?

Although there are no studies I can find specifically to evaluate the effect of exercise on ADT-induced cardiovascular events, there is a large body of evidence supporting the role of physical activity in the prevention and management of cardiovascular disease in the general population. (Thompson et. Al 2003. Osteoporosis ( bone fragility), is a major side effect of ADT can lead to bone fractures, and bone fractures lead to 37% of deaths in older men. (Ebeling; 2008) A study of 8,833 men aged 18–64.9 years used computed tomography to show an inverse relationship between adiposity (BMI and visceral and subcutaneous adiposity) and bone quality (Zhang et al. 2015)Studies show that resistance training in older men and women, where only high-intensity, and not moderate-intensity, strength training resulted in increased bone mineral density. (Vincent et al. 2002)
METABOLIC SYNDROME ADT During course of Treatment
Metabolic syndrome defined by weight gain, especially waist gain; fasting glucose 100 mg/dL or higher, peripheral insulin resistance; and increased diabetes risk increase the risk of heart disease and stroke, in addition to diabetes as is a common side effect when ADT. Results from a randomized pilot study assessed the impact of over six months of combined metformin, a low-glycemic-index diet, and exercise in 20 prostate cancer patients at ADT initiation and compared this with 20 men who were on ADT alone. The metformin and exercise group had decreased abdominal girth, weight, BMI, and systolic blood pressure, compared with the group on ADT treatment alone, although insulin-resistant biochemical markers were not significantly different. In this small study, however, it was not possible to separate the metformin and dietary effects from the exercise components. (Nobles et al. 2012)
63 prostate cancer patients were randomized to receive either a 3-month aerobic and resistance exercise program or usual care, concomitant to initiation of ADT. Patients receiving the exercise-based intervention demonstrated significant reductions in ADT-associated metabolic effects, including decreased whole body fat mass, abdominal fat, and percentage fat, compared with the usual care control group. (Cormie et al. 2015).C-reactive protein, an inflammation marker commonly elevated in metabolic syndrome, showed a clinically meaningful reduction in a randomized controlled trial of exercise in 57 men on ADT (Galvão et al. 2010)

Exercise Prescription while on ADT
Exercise four hours a week in moderate to high intensity. Anyone on ADT must include weight resistant exercise, two to three times a week, where you push and pull weight against gravity. Types of exercises used in some studies include:
Leg presses
Leg extensions
Leg curls
Lat pull downs
Biceps curls (with dumbbell)
Triceps extension
These are the main strength training exercises performed on many of the studies listed above showing benefit. Strength training movements Dr. Espinoza strongly recommends include:
- Kettlebell training – Pavel on this video sounds like a military agent. He is the best at kettlebells. In Ghana; Leonard Akoto of Burnitfitness is another guru!
- Squats
- Deadlifts
- Benchpress
- The Press
- Pushups
- Pull-ups
If the above movements and exercises sound foreign to you then consider hiring a physical trainer if able to. Not only can a trainer help you with the movements but also help prevent injuries and the recommended one in Ghana is Leonard Akoto of Burnitfitness centre. If an injury occurs during any movements mentioned above, all bets are off, you will not or cannot get the benefit of the exercise.

Listen up! Prostate cancer has to be fought with courage.
Fear should not stop you from trying and consistently training with the exercises mentioned. Prostate cancer has to be fought with courage. The most important point in doing any of the above exercises is to first master the technique of that movement. That is one of two ways you prevent injuries from doing those exercises. The other is avoiding doing too much weight too soon. You can hire a personal trainer if your pockets allow. Leonard Akoto is a good one and you check him via facebook!
References:
Kenfield SA, Stampfer MJ, Giovannucci E, Chan JM. Physical activity and survival after prostate cancer diagnosis in the health professionals follow-up study. J Clin Oncol. 2011;29(6):726–732.
Gardner JR, Livingston PM, Fraser SF. Effects of exercise on treatment-related adverse effects for patients with prostate cancer receiving androgen-deprivation therapy: a systematic review. J Clin Oncol. 2014;32(4):335–346
Thompson PD, Buchner D, Pina IL, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity) Circulation. 2003;107(24):3109–3116.
Keating NL, O’Malley AJ, Smith MR. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J Clin Oncol. 2006;24(27):4448–4456.
Ebeling PR. Clinical practice. Osteoporosis in men. N Engl J Med. 2008;358(14):1474–1482
Galvão DA, Taaffe DR, Spry N, Joseph D, Newton RU. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: a randomized controlled trial. J Clin Oncol. 2010;28(2):340–347.
Zhang P, Peterson M, Su GL, Wang SC. Visceral adiposity is negatively associated with bone density and muscle attenuation. Am J Clin Nutr. 2015;101(2):337–343.
Vincent KR, Braith RW. Resistance exercise and bone turnover in elderly men and women. Med Sci Sports Exerc. 2002;34(1):17–23.
Nobes JP, Langley SE, Klopper T, Russell-Jones D, Laing RW. A prospective, randomized pilot study evaluating the effects of metformin and lifestyle intervention on patients with prostate cancer receiving androgen deprivation therapy. BJU Int. 2012;109(10):1495–1502.
Cormie P, Galvao DA, Spry N, et al. Can supervise exercise prevent treatment toxicity in patients with prostate cancer initiating androgen-deprivation therapy: a randomized controlled trial. BJU Int. 2015;115(2):256–266
DA, Taaffe DR, Spry N, Joseph D, Newton RU. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: a randomized controlled trial. J Clin Oncol. 2010;28(2):340–347.

 It's alarming how SHS students have the courage to sell marijuana on campus; let...
It's alarming how SHS students have the courage to sell marijuana on campus; let...
 Mahama charges new Auditor-General to be bold, fair and independent
Mahama charges new Auditor-General to be bold, fair and independent
 Dr. Pamela Graham sworn in as Ghana’s first female Auditor-General
Dr. Pamela Graham sworn in as Ghana’s first female Auditor-General
 Government appoints Brig. Gen. Okae-Yeboah to lead nationwide flood mitigation t...
Government appoints Brig. Gen. Okae-Yeboah to lead nationwide flood mitigation t...
 South African Police link killing of Ghanaian national in Cape Town to extortion...
South African Police link killing of Ghanaian national in Cape Town to extortion...
 GMet forecasts moderate rainfall over the weekend
GMet forecasts moderate rainfall over the weekend
 Gov't to build 10 new SHSs, rehabilitate 150 existing ones — Haruna Iddrisu
Gov't to build 10 new SHSs, rehabilitate 150 existing ones — Haruna Iddrisu
 GH¢100m allocated annually for special needs education — Haruna Iddrisu
GH¢100m allocated annually for special needs education — Haruna Iddrisu
 Dada Joe Remix pleads guilty in US Court to multi-million-dollar romance fraud
Dada Joe Remix pleads guilty in US Court to multi-million-dollar romance fraud
