
From muscle mass and libido to bone density and mood, testosterone governs more of male biology than most men realize and its gradual decline after 30 is one of the most consequential, least-discussed processes in men's health
What Is Testosterone?
Testosterone is the primary male sex hormone, belonging to a class of hormones known as androgens. It is produced mainly in the testes specifically in Leydig cells under instruction from the brain. The hypothalamus releases gonadotropin-releasing hormone (GnRH), which signals the pituitary gland to release luteinising hormone (LH), which in turn tells the testes to produce testosterone.
This feedback loop, known as the hypothalamic-pituitary-gonadal (HPG) axis, governs how much testosterone circulates in the bloodstream at any given time.
Small amounts of testosterone are also produced by the adrenal glands in both men and women, but it is men who produce it in quantities sufficient to drive the sweeping physical, psychological, and reproductive changes associated with male biology.
What Testosterone Does
Testosterone is not merely a sex hormone. Its reach extends into nearly every organ system in the male body.
During foetal development, testosterone drives the formation of male reproductive organs. During puberty, it is responsible for testicular and penile growth, the deepening of the voice, the growth of facial and body hair, the broadening of the shoulders, the development of muscle mass, and the maturation of sperm production.
In adult men, testosterone continues to serve multiple functions simultaneously. It maintains libido and sexual function, regulates sperm production, preserves muscle mass and strength, supports bone mineral density, influences red blood cell production, modulates fat distribution particularly the tendency to store fat centrally and plays a significant role in mood regulation, motivation, cognitive sharpness, and energy levels. Men with healthy testosterone levels tend to sleep better, recover faster from physical exertion, and maintain sharper focus.
Normal Levels and How They Are Measured
Testosterone levels are measured through a blood test, typically taken in the morning when levels are naturally at their peak. Results are expressed in nanomoles per litre (nmol/L) or nanograms per decilitre (ng/dL), depending on the laboratory.
The generally accepted normal range for adult men is between 10.4 and 35.7 nmol/L (approximately 300 to 1,000 ng/dL), though reference ranges vary slightly between laboratories and medical bodies. It is important to note that testosterone circulates in two forms: bound testosterone attached to proteins like sex hormone-binding globulin (SHBG) and albumin and free testosterone, which is the biologically active fraction available to tissues. Total testosterone tests measure both; free testosterone tests isolate only the active portion.
A man may have a total testosterone reading within the normal range but still experience symptoms if his free testosterone is low, particularly if SHBG levels are elevated a situation that becomes more common with age.
"Most Men Come to Us Only When the Problem Has Become a Crisis"
At Manhyia District Hospital in Kumasi, in the heart of the Ashanti Region, Dr. Mathias Azure, a physician in the facility's general outpatient department, spoke with this reporter about what he observes on the ground daily.
"The honest truth is that most of the men who come to us with these complaints are already in their late 40s or 50s, and they have been managing the symptoms privately for years," Dr. Mathias Azure said. "They attribute everything to stress, to work, to spiritual attack. By the time they sit in front of me, the problem is not early-stage anymore."
He described the typical presentation: a man in his 50s complaining of fatigue that does not resolve with rest, reduced interest in sex, difficulty concentrating, and unexplained weight gain around the abdomen. "These men are not lazy. They are not depressed in the psychiatric sense. They are hormonally depleted and nobody told them that this was a medical condition that could be investigated and treated."
Asked about the diagnostic pathway available at the district level, Dr. Mathias Azure was candid. "We do not have endocrinologists here. What we can do is take a history, do a clinical examination, and refer for blood tests. The challenge is cost a full hormonal panel is not cheap for the average Ghanaian patient, and it is not covered under NHIS for this indication. So many men are managed symptomatically without ever getting the proper diagnosis."
He noted that when hormonal testing is done and low testosterone is confirmed, the options available at district hospital level are limited. "We can counsel on lifestyle weight loss, exercise, sleep, alcohol reduction. For replacement therapy, we typically refer upward, to a teaching hospital or a specialist. The system is not designed to manage this at the primary level, which is a gap."
The Decline Begins at 30
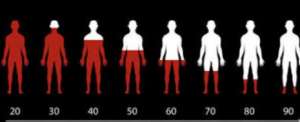
Peak testosterone production occurs in late adolescence and early adulthood, typically between the ages of 18 and 25. From approximately age 30 onwards, testosterone levels decline at an average rate of one to two percent per year. This gradual process sometimes called andropause or late-onset hypogonadism is not a sudden drop but a slow erosion that many men do not notice until symptoms have accumulated over years.
By the time a man reaches his 50s, his testosterone levels may be 20 to 30 percent lower than they were in his 20s. By his 70s, the decline may be 40 to 50 percent. For some men, the fall is steeper; for others, more gradual. Genetics, lifestyle, and underlying health conditions all influence the trajectory.
Unlike the relatively abrupt hormonal transition women experience at menopause, the male hormonal decline is insidious which is partly why it so often goes unrecognized and unaddressed.
Dr. Mathias Azure made the same point from clinical experience. "Women have menopause there is a name for it, there is awareness about it, there is a protocol. Men have nothing equivalent in public consciousness. The decline is gradual, the symptoms are vague, and the culture discourages men from talking about their health. That is a very dangerous combination."
Symptoms of Declining Testosterone
The symptoms of low testosterone clinically termed hypogonadism when levels fall below the normal threshold span the physical, sexual, psychological, and cognitive domains.
Physically, men may notice a loss of muscle mass even without changes in exercise habits, an increase in body fat particularly around the abdomen, reduced bone density that increases fracture risk, decreased body and facial hair, breast tissue enlargement (gynaecomastia), and reduced testicular size. Fatigue that is disproportionate to activity levels is among the most commonly reported complaints.
Sexually, declining testosterone manifests as reduced libido, erectile dysfunction or difficulty maintaining erections, reduced semen volume, and in some cases infertility. These symptoms are often the first to prompt men to seek medical evaluation, yet they frequently reflect hormonal decline that has been progressing for years.
Psychologically, the effects can be equally disabling. Low testosterone is associated with irritability, depression, anxiety, reduced motivation, poor concentration, and a general flattening of mood and drive. Many men describe a loss of the competitive, goal-directed energy that characterised their earlier adult years. Sleep disturbances including insomnia and reduced sleep quality are also frequently reported.
"The mood symptoms are the ones families notice first," Dr. Mathias Azure observed. "The wife will say: he has changed. He is irritable, withdrawn, not himself. And the man himself may not connect it to a hormonal issue at all. He may think it is depression, or that something is wrong with his marriage, or that he is under spiritual attack. We lose a lot of time that way."
Ageing Complications Beyond Low Testosterone
The complications of testosterone decline do not exist in isolation. They interact with the broader biology of male ageing in ways that compound risk.
Cardiovascular health is affected: testosterone has vasodilatory effects and supports healthy lipid profiles. Its decline is associated with increased risk of metabolic syndrome, insulin resistance, and type 2 diabetes. Men with low testosterone are statistically more likely to develop cardiovascular disease, though the relationship is complex and not fully linear.
Bone health deteriorates significantly. Testosterone is essential for maintaining bone mineral density. Low levels accelerate bone loss, increasing the risk of osteoporosis a condition often mistakenly regarded as exclusively a women's health concern. Men with long-standing low testosterone are at measurably higher risk of fractures, particularly of the hip and spine.
Cognitive decline is an area of growing research interest. Some studies suggest that testosterone plays a neuroprotective role, and that its decline is associated with increased risk of cognitive impairment and Alzheimer's disease, though causality remains debated.
Anaemia can develop, as testosterone stimulates the production of erythropoietin the hormone that triggers red blood cell production. Men with low testosterone may experience fatigue partly because of reduced red blood cell counts.
Dr. Mathias Azure flagged the cardiovascular and metabolic dimension as particularly relevant for his patient population. "In this part of Ghana, we see a lot of hypertension and diabetes in men above 45. What people do not always appreciate is that these conditions and low testosterone feed into each other. Obesity drives down testosterone; low testosterone worsens insulin resistance; insulin resistance accelerates cardiovascular risk. You are dealing with a cluster, not isolated diseases."
Factors That Accelerate the Decline
While some degree of testosterone decline is inevitable with age, several factors can accelerate it significantly. Obesity is among the most important: adipose (fat) tissue contains an enzyme called aromatase that converts testosterone to oestrogen, and excess body fat therefore suppresses testosterone. Chronic stress elevates cortisol, which directly inhibits testosterone production. Poor sleep particularly disrupted or insufficient sleep impairs the nocturnal testosterone pulses that occur during deep sleep cycles.
Alcohol consumption, particularly heavy or chronic drinking, damages Leydig cells and suppresses the HPG axis. Certain medications including opioids, glucocorticoids, and some antidepressants can suppress testosterone. Sedentary lifestyle, nutritional deficiencies (particularly of zinc, vitamin D, and magnesium), and exposure to endocrine-disrupting chemicals found in plastics and pesticides have all been associated with lower testosterone levels.
"Alcohol is a big one here," Dr. Mathias Azure said without hesitation. "A significant number of the men I see who present with these symptoms drink heavily sometimes daily. They do not think of it as a health issue. It is social, it is cultural. But the damage to testicular function from chronic alcohol is real and cumulative. I tell them plainly: every year of heavy drinking is a year you are robbing from your hormonal health."
When to See a Doctor
Men who experience a cluster of the symptoms described above particularly fatigue, reduced libido, loss of muscle mass, mood changes, and cognitive dulling should consult a physician and request a hormonal panel that includes total and free testosterone, LH, FSH, prolactin, and thyroid function. Diagnosis of hypogonadism should not be based on a single reading; guidelines recommend at least two morning blood tests on separate days, given the natural variability of testosterone levels.
"Come early that is my message to men," Dr. Mathias Azure said. "Do not wait until your wife is threatening to leave, or until you cannot climb a flight of stairs without exhaustion. The earlier you come, the more options we have. The earlier we catch the problem, the more reversible it is."
He added a point that resonated beyond the clinical: "There is no shame in this. It is biology. Every man's testosterone will decline. What separates the men who age well from the men who do not is largely whether they took their health seriously when they still had time to act."
Management: Natural and Medical Approaches
The management of declining testosterone depends on severity, symptoms, and individual circumstances. Lifestyle interventions remain the foundation: resistance training consistently raises testosterone levels; adequate sleep supports the nocturnal hormonal surges; weight loss in overweight men can produce substantial rises in testosterone; stress reduction lowers the cortisol that suppresses testosterone; and nutritional optimization particularly ensuring adequate zinc, vitamin D, and healthy fat intake supports the hormonal machinery.
Where lifestyle measures are insufficient, testosterone replacement therapy (TRT) is available in several forms: injections, gels, patches, and implants. TRT can be highly effective in restoring wellbeing, libido, muscle mass, bone density, and mood in men with clinically confirmed hypogonadism, but it is not without risks. It can suppress natural testosterone production, reduce sperm count, raise haematocrit, and has implications for prostate health. TRT should be undertaken only under medical supervision with regular monitoring.
Dr. Mathias Azure acknowledged the limits of what district-level care can offer. "What I can do is counsel, test where the patient can afford it, and refer. The specialist services are at Komfo Anokye, at Korle Bu. That is where the management of confirmed hypogonadism will happen. My role is to identify and refer and to stop men from going to unqualified sources, because that is a real problem. There are people selling testosterone injections in markets and online with no oversight, no dosing guidance, no monitoring. That is dangerous."
A Word for African Men
In many African cultures, discussions of hormonal health, sexual decline, and ageing remain culturally suppressed seen as a sign of weakness or as matters too private for clinical conversation. This silence has real health consequences. Men who attribute the fatigue, irritability, and reduced vigour of testosterone decline to spiritual causes, overwork, or personal failure may spend years suffering conditions that are diagnosable and, in many cases, manageable.
The growing availability of laboratory services across West Africa, including in Ghana and Nigeria, means that hormonal testing is increasingly accessible. Men above the age of 40 and particularly those with the risk factors outlined above should regard hormonal health as an essential component of preventive care, no less important than blood pressure or blood sugar monitoring.
Dr. Mathias Azure put it simply: "We talk openly about malaria, about hypertension, about diabetes. We need to talk just as openly about men's hormonal health. The suffering is real. The solutions exist. The only thing standing in the way is silence."
Conclusion
Testosterone does not merely define male identity at puberty it sustains male health across the entire arc of adult life. Understanding its role, recognizing the signs of its decline, and taking proactive steps to preserve it or address its loss is not vanity. It is, for the modern man who intends to age well, a matter of basic biological literacy. And as Dr. Mathias Azure of Manhyia District Hospital affirms, it is a conversation that Ghana's health system and Ghana's men can no longer afford to postpone.
Mustapha Bature Sallama.
Medical/ Science Communicator,
Private Investigator, Criminal investigation and Intelligence Analysis.
International Conflict Management and Peace Building.USIP
[email protected]
+233-555-275-880

 GWL resumes production at Barekese Water Treatment Plant after completion of rep...
GWL resumes production at Barekese Water Treatment Plant after completion of rep...
 Economic performance most powerful source of Mahama’s goodwill — IEA
Economic performance most powerful source of Mahama’s goodwill — IEA
 Nyinahini SHS assault: Court strikes out case, urges reconciliation
Nyinahini SHS assault: Court strikes out case, urges reconciliation
 Even traffic lights in front of police headquarters are being stolen — Roads Min...
Even traffic lights in front of police headquarters are being stolen — Roads Min...
 One major cause of Ablekuma North rerun violence was lack of security coordinati...
One major cause of Ablekuma North rerun violence was lack of security coordinati...
 BTU Council divided as Chairman rejects parliamentary mediation in VC dispute
BTU Council divided as Chairman rejects parliamentary mediation in VC dispute
 Roads Ministry needs 1,000 additional staff — Governs Agbodza
Roads Ministry needs 1,000 additional staff — Governs Agbodza
 Stop tweeting and brief Parliament on South Africa situation — Patrick Boamah to...
Stop tweeting and brief Parliament on South Africa situation — Patrick Boamah to...
 Roads Minister reassigns Bogoso–Prestea road project to new contractor over dela...
Roads Minister reassigns Bogoso–Prestea road project to new contractor over dela...
 President Mahama’s approval rate remains positive at 58.9% — IEA survey shows
President Mahama’s approval rate remains positive at 58.9% — IEA survey shows
