
Oral contraceptives also called birth control pills are a safe and reliable option for preventing unwanted pregnancy. Most oral contraceptives contains a combination of 2 types of hormone: an estrogen and a progestin. Both of these hormone are naturally found in the women’s bodies. There are many different types of estrogens and progestin’s, and different types of pills contain different combinations, but they all work similarly. Some pills contain only progestin, sometimes called the mini-pills. The question is who can take oral contraceptive? The most requirement for women taking oral contraceptives is that they must remember to take them every day at approximately the same time of day. Oral contraceptives are not a good form of birth control when doses are missed frequently. Combination oral contraceptives should not be given to women older than 35 years who also smoke, because there is an increased risk of blood clots in these women, or to women who have high blood pressure and heart disease.
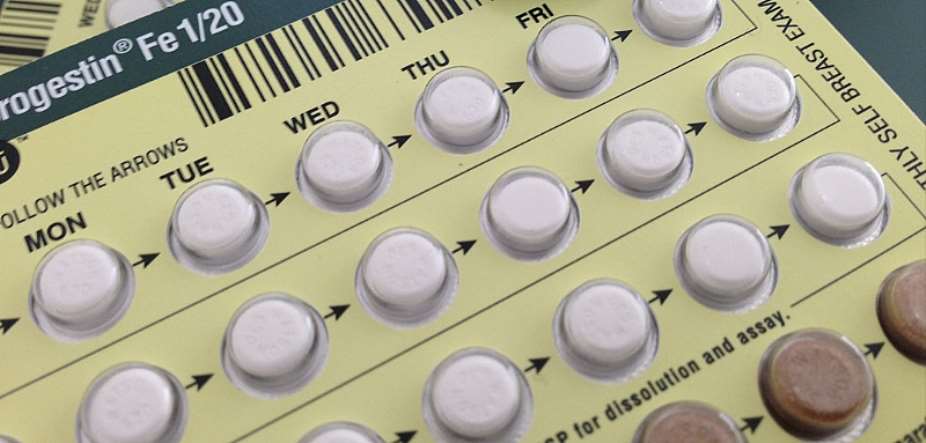
Oral contraceptives are usually prescribed for 4 weeks at a time, with each 4-weeks packet containing 4 to 7 days of hormone-free pills. Women get their period during these hormone-free days. Some preparations have extended or continuous hormone dosing with fewer or no hormone –free days so that women get their periods less than once a month. Oral contraceptives can be started any day of the week and any day of the menstrual cycle.
When oral contraceptives became generally available during the early 1960s, their use increased rapidly, initially in North America and then elsewhere. By 1965, approximately 15 per cent of all married women 15 to 44 years of age in the United states were taking oral contraceptives; by 1973, this figure had increased to 25 per cent, or about 6.6 million. Use in the United states peaked during the mid-1970s but has continued to increase in many other countries. Worldwide, it is estimated that about 54 million women were using oral contraceptives by 1977.
The evidence for and against the association of oral contraceptives of with vascular disease is reviewed, along with the possible pathophysiologic mechanisms for such an association, including effects on coagulation, circulating lipoproteins, and glucose metabolism. The new, low-dose estrogen OCs appear to affect coagulation minimally, and anticoagulant, as well as procoagulant effects, have been documented. Such concomitant factors as cigarette smoking, obesity, a family history of thrombosis, lack of physical activity and blood type influence coagulation more strongly correlated with the levels and pattern of circulating lipoproteins. The estrogen components of OCs have a favorable effect on lipids while the effect of progestin’s. Particularly potent androgenic progestin’s, is unfavorable and could be significant. OCs containing high-dose androgenic progestin’s can produce abnormal glucose tolerance resulting in increased cardiovascular risk. Low-dose OCs are associated with early, transient breakthrough bleeding. However, educating patients in the management of breakthrough bleeding can help reduce the number of women who must be switched to higher dose OCs. Epidermiologic evidence confirms the safety of low-dose OCs. By selecting patients carefully, the risk of vascular disease from oral contraception can be reduced to very low levels. In this review of cardiovascular effects of oral contraceptives (OCs), the risks are identified from 2prospective cohort studies as 19/10,000 woman years for the risk of thrombosis or thromboembolism. 11 of 19 were superficial thrombosis and 8 were deep vein thrombosis or pulmonary embolism. For women with no risk factors, the risk was 2.0 for superficial thrombosis and 4.0 for deep vein thrombosis.
We examined the effects of past use of oral contraceptives on risks of cardiovascular disease prospectively in the nurses health study cohort. The 119,061 participants were 30 to 35 years old and free of coronary disease or stroke in 1976. They provided information on biennial questionnaires and were followed for 8 years. There were 380 nonfatal myocardial infarctions and 105 deaths from coronary disease, 282 strokes and 48 other cardiovascular deaths. We observed virtually no differences in the rates of various cardiovascular diseases between never and past users of oral contraceptives, regardless of duration of use or time since last use. For majority coronary disease, the relative risk was 0.8(95% confidence intervals, 0.6 to 1.0). A quantitative meta-analysis of 13 studies yielded an estimated relative risk of 1.01(95% confidence intervals, 0.91 to 1.13) for coronary heart disease. Past use of oral contraceptives has little or no impact on risks of subsequent cardiovascular diseases. Macrovascular diseases, especially coronary heart diseases, have found to be linked to glucose intolerance. Insulin resistance in respect to glucose uptake in peripheral tissues seems to play an important role in the development of glucose intolerance, since subjects with coronary heart disease mainly are hyperinsulinemic. Insulin resistance may induce not only glucose intolerance but also hypertension, obesity, and dyslipoproteinemia (high very low-density lipoprotein and low high-density lipoprotein values), all variables that add to the risk of coronary heart disease. On the basis of these findings, a new syndrome has been postulated-syndrome X. This syndrome may be caused by inherited insulin resistance in skeletal muscles, and secondary to that arterial hypertention, obesity, and dyslipoproteinemia may develop. Insulin resistance in noninsulin-dependent diabetic persons and in hypertensive subjects is located in the skeletal muscles, where insulin’s ability to promote nonoxidative glucose metabolism is reduced. The key enzyme in this pathway, glycogen synthase, is proposed as the casual defect responsible for the insulin resistance state, at least in noninsulin-dependent diabetic patients. The pill (sex steroids) may induce a clinical situation that is similar to syndrome X. however, it is important to emphasize that many more studies are needed to substantiate these hypothetical mechanisms behind coronary heart disease.
ACKNOWLEDGMENT
Dr. Kingsley Preko
Dr. A. T. Derrick
PHILIPA DANYOMAH
LEVEL 200
PHYSICIAN ASSISTANT STUDENT
UNIVERSITY OF CAPE COAST
 This IMANI job no dey pap; the people you are fighting for are always fighting y...
This IMANI job no dey pap; the people you are fighting for are always fighting y...
 Prof. Naana Opoku-Agyemang has changed; you can see a certain sense of urgency –...
Prof. Naana Opoku-Agyemang has changed; you can see a certain sense of urgency –...
 MFWA Executive Director slams Akoma FM for engaging in ‘irresponsible’ media pra...
MFWA Executive Director slams Akoma FM for engaging in ‘irresponsible’ media pra...
 ‘Women must become millionaires too’ — Prof Jane Naana on establishment of Women...
‘Women must become millionaires too’ — Prof Jane Naana on establishment of Women...
 Some believe only in Ghanaian votes, not Ghana — Kofi Asare jabs politicians
Some believe only in Ghanaian votes, not Ghana — Kofi Asare jabs politicians
 Plan to make BEST sole aggregator of Sentuo Oil Refinery will create market chal...
Plan to make BEST sole aggregator of Sentuo Oil Refinery will create market chal...
 2024 elections: I can't have the man I removed from office as my successor — Aku...
2024 elections: I can't have the man I removed from office as my successor — Aku...
 2024 Elections: Immediate-past NPP Germany Branch Chairman garners massive votes...
2024 Elections: Immediate-past NPP Germany Branch Chairman garners massive votes...
 Gov’t focused on making Ghana energy self-sufficient, eco-friendly – Akufo-Addo
Gov’t focused on making Ghana energy self-sufficient, eco-friendly – Akufo-Addo
 April 25: Cedi sells at GHS13.74 to $1, GHS13.14 on BoG interbank
April 25: Cedi sells at GHS13.74 to $1, GHS13.14 on BoG interbank
