
DIZZINESS
Dizziness is the general term used to describe the feeling of lack of balance when standing or when moving the head
Anatomy
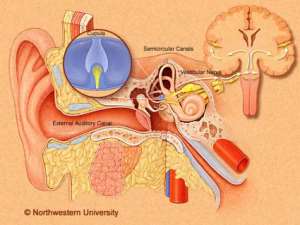
Anatomically, the ear has been divided into 3: the outer, middle and inner ear.
The inner ear is made up of the cochlea and the vestibular system. The cochlea is involved with hearing. The vestibular system “the organs for normal balance” detects movement and helps with balance.
The vestibular system is made up of a network of fluid filled tubes called the semicircular canals and the ,vestibule which consist of the utricle and saccule.
The utricle and saccule have calcium carbonate crystals (otoliths) which when displaced by linear movements, set up nerve signals that pass through the vestibular nerve to the vestibular centers in the brain.
The three semicircular canals contain receptors that detect angular(non-linear) head movements.
Pathophysiology
Any disturbances in either of the two (left and right) vestibular organs, or the nerves that send signals to the balance centers in the brain, as well as failure of the brain to coordinate input signals from the vestibular organs, with signals from the eyes, muscles and joints, result in a sense of imbalance.
VERTIGO.
Vertigo is the most common form of dizziness.
Vertigo is defined as the sensation of movement (usually a spinning motion) of either self or the environment.
Vertigo is broken down into central (when pathology is in the brain, precisely, the brainstem or cerebellum) and peripheral (when the pathology involves the vestibular system).
PERIPHERAL VERTIGO
(1) BENIGN PAROXYSMAL VERTIGO (BPPV)
This is the most common type of vertigo.
The most common cause in people under 50 is head trauma.
In older people, the most common causes are degenerations in the vestibular systems.
BPPV becomes more common with advancing age.
Utricle and saccule have sensory receptors that contain small calcium carbonate crystals which help to detect small linear movements of the head.
Occasionally, calcium carbonate crystals may dislodge from the utricle (following head injury, infections or degenerative lesions) and migrate into the semicircular canals. Linear head motions induce movement of these crystal within the semicircular canals, falsely sending signals to the vestibular nerve on that side. This causes signal imbalance between the left and right vestibular nerves, and vertigo, results.
The symptoms are usually precipitated by change in position of the head with respect to gravity. Getting out of bed, turning in bed, tipping the head back to look up (top shelf vertigo) or bending forward.
The dizziness (vertigo) last 10-30 seconds only.
The dizziness may recur and may last for months
SYMPTOMS OF VERTIGO
. Sensation of motion
. Nausea and vomiting
. Sweating
. Abnormal eye movements (nystagmus) in all planes: horizontal-vertical-torsional. The nystagmus decreases with fixation, and with time, lasting less than 1 minute and exhibit latency after maneuvers.
DIAGNOSIS
Dix-Hallpike maneuver, which orients the head to align the posterior canal with gravitational forces, provoking the classic vertigo. This maneuver helps to differentiate the central from peripheral causes of vertigo. In those with BPPV, this test elicits the following characteristic of nystagmus
. latency of 2-40seconds
. Duration <1 minute
. Fatigability
. Direction of nystagmus, may be vertical, horizontal or torsional.
TREATMENT
-
Particle Repositioning procedures, done by doctors in their offices. Epley’s maneuver involves, the doctor, sequentially moving your head in 4 positions, staying in each position for about half a minute. This procedure, dislodges the crystals from the semicircular canals
-
Medications do not treat BPPV, they are used to relieve symptoms only. The medications include (a). Antihistamines block histamine release in the vestibular-cerebellar pathways. Meclizine 25 mg orally every 6 hours.
(b). Vestibular suppressants act on GABA receptors to block nerve transmission: Diazepam1mg orally twice daily and clonazepam 0.25mg BID.
(c). Antiemetics: The phenothiazines are effective against vomiting: prochlorperazine 5-10mg orally three times daily
(d). Vitamin D supplements may benefit those with BPPV, and low vitamin D levels.
(2) VESTIBULAR NEURITIS
The vestibular nerve carries information from the inner ear, about head movements. Inflammation due to Viral infection of one of the 2 vestibular nerve causes imbalance between the signals from the two sides and vertigo results. The vertigo lasts for days until the inflammation subsides.
The symptoms include: vertigo, nausea, imbalance.
When hearing symptoms (tinnitus, hearing loss) accompany vestibular neuritis, the term labyrinthitis is used
Treatment of Vestibular Neuritis:
Antiemetics: Phenergan 5-10 mg x3 daily
Vestibular suppressants Diazepam 1mg twice daily
Antihistamine: meclizine 25mg every 6 hours
(3) MENIERE’S DISEASE. (Idiopathic Endolymph Hydrops)
When vertigo is associated with ringing in the ears and hearing loss, it may be related to Meniere’s disease
Occasionally, as a response to Inflammation, excess fluid is produced by the vestibular organs and the subsequent rise in fluid pressure may interfere with normal balance and hearing signals between the inner ear and the brain.
When this happens, the individual may have episodic symptoms of vertigo, low pitched hearing loss, ringing/buzzing/roaring in the ears and a sensation of fullness in the affected ear.
An episode may last for 20 minutes to several hours. Permanent hearing loss, eventually occurs, if condition is left untreated.
Diagnosis of Meniere’s Disease: from clinical history
. Two or more episodes of vertigo lasting at least, 20 minutes each
. Ringing/roaring/ buzzing in the ear
. Temporary hearing loss
. A feeling of fullness in the ear.
Treatment of Meniere’s disease
. Dizziness: meclizine, lorazepam, diazepam
. Fluid buildup: diuretics and restrictions on salt intake
. Surgery to decompress the endolymphatic sac
If this condition is not treated, permanent hearing loss may occur
CENTRAL VERTIGO
Central vertigo, is usually an emergency.
This may occur in people with hypertension, diabetes, high cholesterol, multiple sclerosis and in older persons. The vertigo usually, may be due to a stroke that occurs in the brainstem and cerebellum.
Other causes of central vertigo include: Migraine, Multiple sclerosis.
Affected persons may present with dizziness, associated with
. Difficulty with swallowing
. Double vision or visual loss
. Difficulty speaking
. Hearing loss
. Leg or arm weakness
. Gait unsteadiness, Difficulty walking and or falling
. Numbness tinging and Weakness
. Dix-Hallpike test shows Pure vertical nystagmus that remains unchanged with fixation and last longer than a minute.
Diagnosis of Central Vertigo.
MRI of the brain
Such dizziness are life threatening conditions that require immediate medical attention.
NON-VERTIGINOUS DIZZINESS
1. LIGHTHEADEDNESS/PRESYNCOPE (“Faint” feelings of dizziness)
Any condition that causes a decrease in cerebral perfusion may cause a feeling of about to faint or “pass out”. They include
. heart arrhythmias, which may lead to syncope (fainting spells)
. low blood pressure,
. diseases of the heart valves and other situations like
. dehydration, and bleeding
. emotional stress
. anxiety
. extreme fear
. hyperventilation
. pain
. hunger.
Affected persons may have dizziness, associated with nausea, warmth and tunnel vision but no feeling of movement of self or the surroundings.
The condition is known as presyncope, as there is no change in consciousness or faint spells.
Lightheadedness goes away or improves, on lying down.
Treatment is geared toward the underlying causes
DISEQUILIBRIUM/IMBALANCE
Disequilibrium, usually occurs in the elderly population who experience imbalance or unsteady gait on walking or standing.
Disequilibrium is due to:
. neurological degenerative diseases like Parkinson’s disease,
. medications toxicity,
. Poor eyesight,
. Poor hearing,
. Poor sensation to touch and position.
The problem ceases when they sit or lie down
WHEN TO SEE A DOCTOR
The following symptoms, associated with dizziness, are emergency conditions.
. Fever
. Double, blurry vision, or Abnormal eye movement
. Sudden or severe headache
. Change in consciousness or not acting or reacting appropriately.
. Difficulty speaking
. Unsteady gait, difficulty walking, and or falling.
. Weakness, numbness and tingling in an arm or a leg
. Difficulty swallowing
. Loss of hearing
. Any dizziness that is worrisome.
 We’ll no longer tolerate your empty, unwarranted attacks – TUC blasts Prof Adei
We’ll no longer tolerate your empty, unwarranted attacks – TUC blasts Prof Adei
 Bawumia donates GHc200,000 to support Madina fire victims
Bawumia donates GHc200,000 to support Madina fire victims
 IMF to disburse US$360million third tranche to Ghana without creditors MoU
IMF to disburse US$360million third tranche to Ghana without creditors MoU
 Truck owner share insights into train collision incident
Truck owner share insights into train collision incident
 Paramount chief of Bassare Traditional Area passes on
Paramount chief of Bassare Traditional Area passes on
 Two teachers in court over alleged illegal possession of BECE papers
Two teachers in court over alleged illegal possession of BECE papers
 Sunyani: Victim allegedly shot by traditional warriors appeals for justice
Sunyani: Victim allegedly shot by traditional warriors appeals for justice
 Mahama vows to scrap teacher licensure exams, review Free SHS policy
Mahama vows to scrap teacher licensure exams, review Free SHS policy
 Government will replace burnt Madina shops with a new three-story, 120-store fac...
Government will replace burnt Madina shops with a new three-story, 120-store fac...
